Epidural Steroid Injections
Lumbar epidural steroid injections are controversial in when they are given, where they are given, why they are given, how often they should be given and what medications work best. Whatever position you may have personally as a physician, you usually can find support in the literature. As such, my recommendations are based on both the literature and my experience over the last 20 years with these types of injections.
First, Where They Are Given “Epidural” means outside the dura which is a sac-like tissue containing of the nerve roots. The nerves float in the cerebrospinal fluid (CSF) within the dural sac.
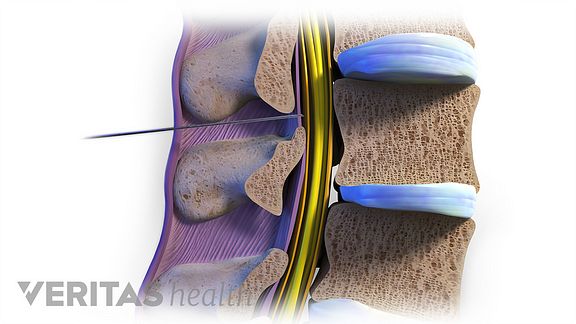
ESI’s are given near but outside the dural sac. Generally, ESI’s are given in one of 3 ways: interlaminar, transforaminal and caudally.
Interlaminar injections are given in the midline between the spinous processes of the spine, usually at the L4-5 level and have effect over a few levels above and below L4-5. These injections can be done in the office setting but can also be performed in a surgery center with fluoroscopy. This kind of epidural is the kind one would use in pregnancy, although the medication would be different (a numbing or pain medication rather than an inflammation medication like a steroid).
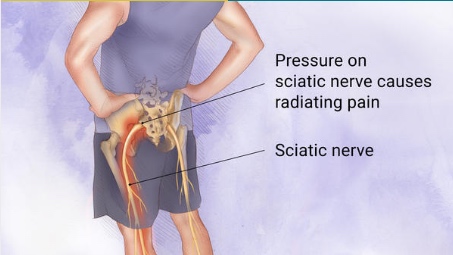
Transforaminal ESI’s are given where the nerve root exits the neuroforamen (the holes on the side of the spine) and goes into the nerves of the leg, for example the sciatic nerve.
These types of injections are done by a lateral approach and targets a specific nerve. So a right L4-5 transforaminal ESI would target the right L5 nerve. Other nerves generally would not be affected.
Transforaminal injections are done with fluoroscopy and often in a surgery center setting. If you are not sure if the pain radiating into a patient’s leg is from a particular nerve, a specific transforaminal injection can help you make the diagnosis. Learn more about Transforaminal Epidural Steroid Injections here!
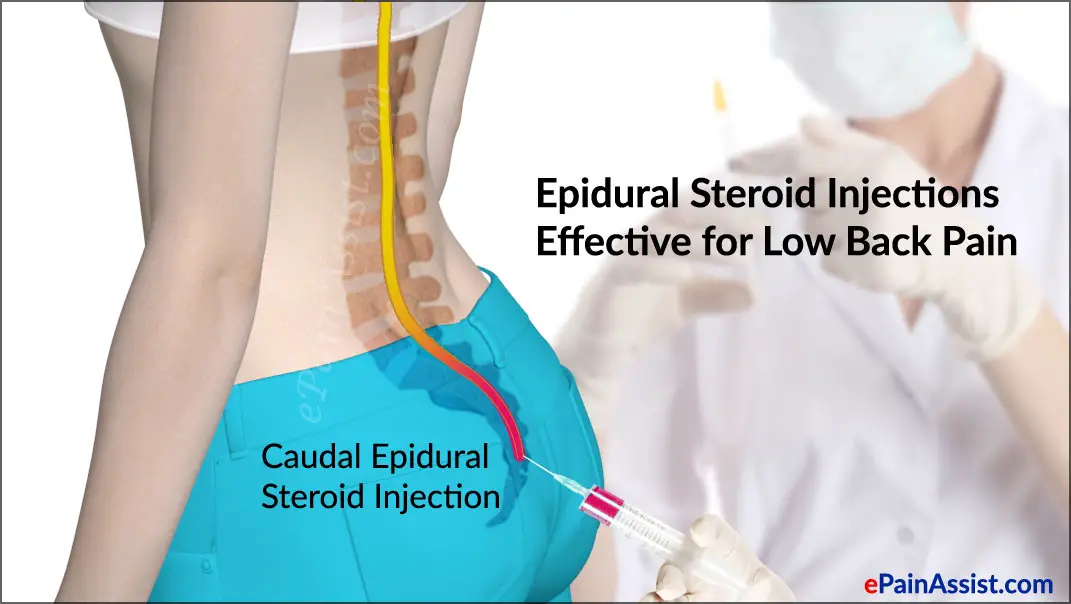
Caudal ESI’s are given below the sacrum and a catheter is threaded cranially toward the lumbar spine. As with the interlaminar injection, the medication given can affect a few levels . Generally, it is useful if a patient has had surgery as scarring can make it difficult to give an interlaminar injection. These types of injections are given in a surgery center with fluoroscopy so the catheter can be visualized.
Next, Why and When They Are Given
It depends on what you are treating and what you want to accomplish. ESI’s are generally given for symptoms of leg pain. Sciatic pain from a lumbar disc herniation usually causes burning pain down the leg, past the knee and into the foot.
Disc herniation pain will usually improve with non-surgical care within 6 weeks to 3 months. The reason to do an ESI is to decrease inflammation and help the pain to resolve more quickly. An ESI done any of the above 3 ways would be effective, but the transforaminal injection may be more specific to a particular irritated nerve.
Generally, if a patient is not improving in 6 weeks with sciatic pain from a disk herniation I will recommend an ESI. If a patient does not improve after the first injection then a second is likely to help about 50% of the time in my experience. If a second is not effective, then a third is not likely to help significantly in my experience.
Furthermore, if the pain is not improved or improving by 3 months then surgery should be considered. The reason for this is because the results for surgery are best before the 6 month period. Before 6 months, the nerve is less likely to be injured and the current literature supports this view. So rarely will I recommend a series of injections with a herniation.
In my opinion, 95% of patients with disc herniation sciatica will improve without surgery. Most improve within 3 months. But If the patient is not improving by 3 months after 1 or 2 injections, then they are unlikely to improve after the 3rd or 4th. More injections can lead to unnecessary delay and residual nerve damage. Better to fix the problem between 3 to 6 months and get the patient better quicker.
For arthritic conditions, with arthritic stenosis at multiple levels, ESI’s can be effective. Arthritic stenosis is a chronic condition. The ESI can give relief for a few moths or more. There are different recommendations out there, but about 3 ESI’s per year is likely safe if they are improving the leg symptoms.
Leg pain from arthritic stenosis is different than disc herniation sciatic pain. It usually involves a burning pain and numbness from the buttocks into the back of the thighs. Pain rarely extends below the knee.
Stenosis pain is usually aggravated by walking and relived by bending forward and sitting down. Interlaminar and caudal ESI’s are the typical ones used. Ultimately, a surgical decompression such as a laminectomy may be needed if the ESI’s are no longer effective or do not last.
And Lastly the Medication Generally, a steroid medication is used to provide longer term decrease in inflammation and pain. There are studies to suggest that just injection saline is as effective as steroids. Most physicians will still use steroids for the anti- inflammatory effects. You can inject other substances, such as homeopathic medications, with anti-inflammatory effects as well as PRP from a patients own blood that also has anti-inflammatory effects. Some physicians are strong promoters of these types of injections but in reality the results warrant further study.
By Robert Nucci, MD

Robert C. Nucci, MD
Board Certified Orthopedic Spine Surgeon
Tampa, FL